
Pioneering Nationwide Achievement |Sir Run Run Shaw Hospital Affiliated to Zhejiang University School of Medicine Successfully Treats a Patient with Complex Tricuspid Valve Disease Using K-Clip®
Recently, the team led by Professor Fu Guosheng, including Director Yu Feicheng and Physician Zhu Jun from Sir Run Run Shaw Hospital Affiliated to Zhejiang University School of Medicine, in collaboration with the team of Director Wang Bei and Physician Yu Chan from the Department of Ultrasound and the Department of Anesthesiology, successfully treated a patient with the K-Clip® transcatheter tricuspid valve repair technology, marking another major breakthrough in the field of minimally invasive treatment for valvular heart diseases!
The patient admitted this time had myxomatous degeneration of the tricuspid valve leaflets, mild prolapse-like changes of the valve body, and mild Barlow-like changes. Such complex anatomical structures posed considerable challenges to the treatment. Faced with this difficulty, the team, relying on profound clinical experience, precise diagnosis and treatment standards, and an excellent grasp of cardiac anatomical structures, successfully applied the K-Clip® technology to treat the patient. This technology not only perfectly avoids the disadvantages of traditional open surgery such as severe trauma and slow recovery, but also shows significant minimally invasive advantages in the adaptability to complex lesions, accurately realizing valve function repair and laying a solid anatomical foundation for the patient's rapid postoperative recovery. This successful case is a powerful testament to the team's technical strength and further confirms the clinical value of the K-Clip® technology in the treatment of complex tricuspid valve lesions!


Patient Profile:
Female patient with chronic heart failure, severe tricuspid insufficiency (AFTR 4+ suspected) complicated with moderate to severe pulmonary arterial hypertension.
Preoperative Evaluation
Ultrasound Evaluation:
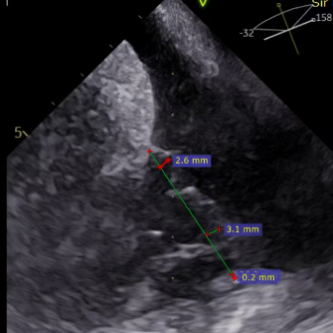
- Type valve with type IIIb quadricuspid malformation and severe insufficiency (mean vena contracta: 7.4mm).
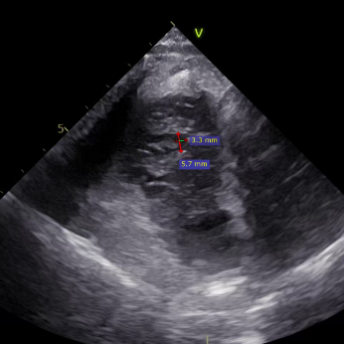
- Regurgitation orifices located at the anteroseptal and posteroseptal commissures, with a 5.7×3.3mm gap detected in the center.
- Myxomatous degeneration of tricuspid valve leaflets with mild prolapse-like changes of the valve body and mild Barlow-like changes.
- No obvious dilatation of the tricuspid annulus (mean annulus diameter: 33mm).
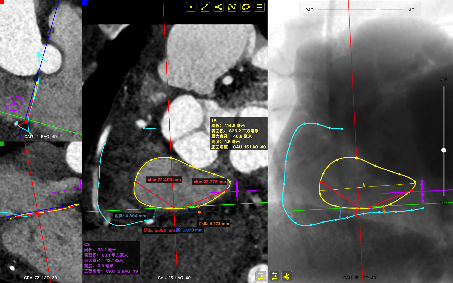
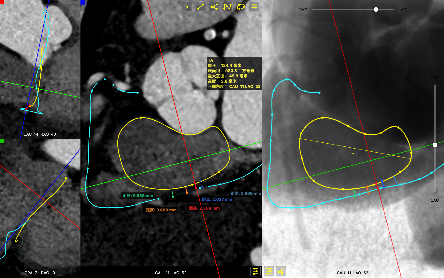
CTA Evaluation:
- Diastolic circumference of the tricuspid annulus: 124mm, area: 983mm² (little change in circumference and area between systole and diastole).
- The closest distance between the right coronary artery (RCA) and the tricuspid annulus (TA) at the posterior annulus during systole is 2.5mm (the target of clip screw deployment can be adjusted to avoid injury).
- Coronary distance >3mm during diastole. Low risk of coronary impact.
- Optimal fluoroscopic projection: Tricuspid valve short-axis CAU15, LAO40.
- Preliminary strategy: one 12T K-Clip® at the posteroseptal commissure and one 12T K-Clip® at the anteroposterior commissure.
Surgical Strategy
Based on profound accumulation in cardiac anatomy and minimally invasive intervention, Professor Yu Feicheng integrated multi-dimensional imaging data from preoperative ultrasound and CT, combined with refined analysis of the patient's cardiac valve anatomical structure, and tailored a targeted treatment plan: a dual-point targeted implantation strategy was recommended, with 12T K-Clip® devices implanted at the septal portion of the posterior leaflet and the anteroposterior commissure respectively.
The core advantages of this treatment plan stem from the unique characteristics of the K-Clip® technology: First, it features excellent minimal invasiveness, eliminating the need for thoracotomy, which can minimize surgical trauma to the patient's body, reduce the risk of intraoperative bleeding and postoperative complications, and lay a foundation for the patient's rapid recovery. Second, it has precise targeted positioning capability, relying on the core design of the technology to achieve accurate implantation and fixation of the device at the target site. Supported by this technology, the tricuspid annulus is reduced, the leaflet coaptation is significantly improved, the pathogenesis of tricuspid regurgitation is blocked from the anatomical root, which provides a key structural guarantee for the recovery of the patient's cardiac function after surgery and greatly improves the therapeutic effect and prognosis quality.
Surgical Procedure
After the patient was placed under general anesthesia, the jugular vein was punctured intraoperatively to establish surgical access. An 18Fr delivery sheath was advanced along a stiff guidewire to the mid-inferior right atrium, and the delivery system was introduced under ultrasound guidance. A 12T K-Clip® device was implanted at the posteroseptal commissure and another 12T K-Clip® device at the anteroposterior commissure respectively. The angle between the device and the annulus plane was adjusted through catheter deflection and rotation to direct the tip of the clip device to the target position. Under ultrasound MPR mode, the anchoring screw was deployed into the annulus. After confirming stable traction, the clamping arms were opened and apposed to the annulus, followed by retraction of the anchoring component to close the clamping arms for annuloplasty. The surgical effect was evaluated as satisfactory, and the clip components were then released.
The delivery system enters the right atrium (RA) via the superior vena cava (SVC)
Deployment of the anchoring component under the MPR view
Opening the clamping arms, adjusting the orientation and apposing to the annulus
Closing the clip
Efficacy evaluation after implantation of the first clip
Implanting the second clip at the anteroposterior commissure following the same procedure
Surgical Outcome
Regurgitation Outcome:
Critical regurgitation (5+) reduced to moderate to severe regurgitation (3+).
Preoperative critical regurgitation (5+)
Postoperative moderate to severe regurgitation (3+)
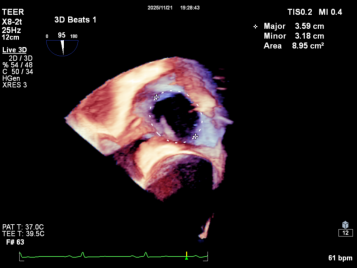
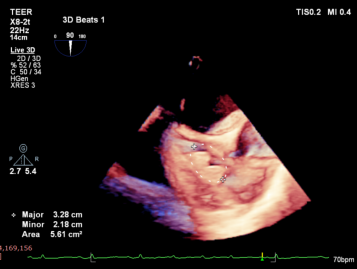
Annuloplasty Outcome:
Summary
The K-Clip® transcatheter tricuspid valve annuloplasty adopts a unique physiological annuloplasty technology with no damage to native valve leaflets. Even in the face of complex anatomical structures such as myxomatous degeneration of tricuspid valve leaflets, mild prolapse of the valve body and mild balloon-like changes, this technology can still accurately reduce the annulus and complete annulus remodeling.
The procedure is performed with precise manipulation under real-time ultrasound guidance, providing a new minimally invasive and reliable treatment pathway for high-risk patients.
This technology breaks through the limitations of traditional surgery for complex lesions, especially opening a safe and effective intervention window for the vulnerable group of elderly patients with multiple comorbidities, showing broad clinical application prospects.
Team of the Cardiac Valve Intervention Center, Sir Run Run Shaw Hospital Affiliated to Zhejiang University School of Medicine
Under the leadership of Professor Fu Guosheng, the sub-specialty team for interventional treatment of valvular heart diseases was established in 2017. The Cardiac Valve Intervention Center of the hospital was officially founded in 2021, realizing multidisciplinary collaboration and resource integration. The team members work closely together with proficient skills, providing standardized diagnosis and treatment for valvular heart diseases and continuously improving the quantity and quality of treatments. The center has carried out a variety of transcatheter aortic valve replacement (TAVR) procedures through different approaches including femoral artery, carotid artery and apical approach; TAVR for critically ill patients under ECMO support; concurrent coronary PCI and TAVR under coronary protection for high-risk patients; TAVR with cerebral protection devices; emergency TAVR, with more than 700 cases completed to date. It has also performed transcatheter edge-to-edge repair (TEER) of the mitral valve, with a total of more than 180 cases. In 2021, the center was designated as one of the "First Batch of Structural Heart Disease (Valvular Heart Disease) Interventional Training Bases by the National Health Commission Hospital Management Research Institute." In 2022, it was honored as a "Benchmark Team for Valve Centers" by the Valvular Heart Disease Interventional Center. In 2023, it was certified as one of the first batch of Valvular Heart Disease Interventional Centers.
专家简介
Expert Profile

Fu Guosheng
Sir Run Run Shaw Hospital Affiliated to Zhejiang University School of Medicine

Yu Feicheng
Sir Run Run Shaw Hospital Affiliated to Zhejiang University School of Medicine

Zhu Jun
Sir Run Run Shaw Hospital Affiliated to Zhejiang University School of Medicine

Yu Chan
Sir Run Run Shaw Hospital Affiliated to Zhejiang University School of Medicine

K-Clip® Transcatheter Tricuspid Annuloplasty System
1. Transvascular puncture approach, minimally invasive, with an 18Fr outer sheath diameter.
2. Simple operation, all steps performed on the atrial side, short learning curve.
3. All steps reversible before deployment, ensuring controlled procedural outcomes.
4. Physiological annuloplasty technique, preserving native leaflets without damage.

K-Clip®经导管三尖瓣环成形系统:
1、经血管穿刺入路,损伤小,鞘管外径18Fr。
2、操作简单,均在心房面完成,学习曲线短。
3、解离前所有操作步骤可逆,手术效果可控。
4、生理性环缩技术,无损原生瓣叶。

