Pioneering Nationwide Achievement | Qingdao Municipal Hospital Applies K-Clip® for Precise Treatment of Severe Tricuspid Regurgitation, Opening a New Chapter in Interventional Therapy
Recently, the Valve Interventional Team of the Heart Center at Qingdao Municipal Hospital (East Campus), led by Professor Shao Yibing, Vice President and Director of the Heart Center, including Professor Xia Wei (Cardiology), Professor Niu Zhaozhuo (Cardiac Surgery), and Professor Chu Qiang (Cardiac Ultrasound), in collaboration with the Anesthesiology Department, Operating Room, and other related departments, successfully completed a challenging transcatheter tricuspid valve annuloplasty (TTVA) procedure using the domestic innovative device K-Clip®. The patient suffered from massive tricuspid regurgitation, a giant right atrium, and had a relatively elongated and redundant posterior leaflet hinge area posing a risk of perforation. Post-procedure, the severity of tricuspid regurgitation was significantly reduced, symptoms were alleviated, and the surgical outcome was satisfactory. This breakthrough procedure at Qingdao Municipal Hospital fills a technological gap in the Qingdao region. It not only demonstrates the hospital's robust multidisciplinary collaboration capability in managing high-risk complex valvular heart disease but also provides high-risk patients with moderate-to-severe tricuspid regurgitation in the Qingdao area access to minimally invasive and effective treatment close to home.



Patient Profile
70-year-old male
Present Illness: 1. Acute exacerbation of chronic heart failure; 2. Rheumatic heart disease, status post mechanical mitral valve replacement, status post mechanical aortic valve replacement, tricuspid regurgitation; 3. Coronary atherosclerotic heart disease, status post coronary artery stent implantation, NYHA Class III; 4. Hypertension Grade 3 (very high risk); 5. Varicose veins of lower extremities; 6. Chronic thromboembolic pulmonary hypertension; 7. Anemia; 8. Chronic congestive liver damage; 9. Persistent atrial fibrillation; 10. Premature ventricular contractions. The patient experienced chest tightness and shortness of breath upon activity for over 2 years, relieved after about 5 minutes of rest. Two weeks ago, the chest tightness worsened with activity, accompanied by worsening lower extremity edema and fatigue.
Past Medical History: History of coronary heart disease, underwent coronary angiography and received one stent in the RCA in 2024; History of "atrial fibrillation" for over 20 years; History of "rheumatic heart disease" for over 30 years, underwent "aortic and mitral valve replacement" 20 years ago; Varicose veins in the left lower extremity, underwent surgery in 2020; Diagnosed with pulmonary microvascular embolism and "chronic thromboembolic pulmonary hypertension" in January 2025.
Preoperative Assessment
1. The risk of intraoperative coronary artery compromise is low. During diastole, the hinge region of the posterior annulus is relatively redundant, with a thickness of 2.7 mm (risk of perforation during screw deployment).
2. Optimal fluoroscopic projection: short-axis view of tricuspid valve, LAO 57°, CAU 11°.
3. Surgical expectation: reduction of regurgitation in the posteroseptal and central regions; favorable anatomy, with an expected reduction of 2–3 grades.
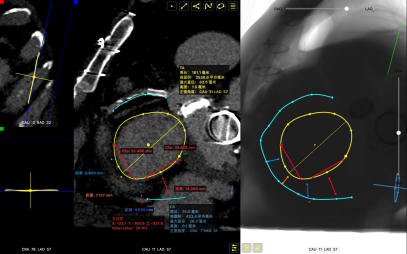
CTA Assessment: 1. Status post mechanical aortic and mitral valve replacement; 2. Tricuspid annular dilation (mean annulus diameter 46.5mm), massive tricuspid regurgitation (6+, mean vena contracta 21.8mm), giant right atrium, wide central gap 11.3mm; 3. Regurgitant orifices: Antero-septal + Central + Postero-septal. No significant leaflet prolapse or tethering observed.
Surgical Procedure
After the patient was placed under general anesthesia, the jugular vein was punctured intraoperatively to establish access. An 18Fr delivery sheath was advanced along the stiff guidewire to the mid‑inferior right atrium. Under ultrasound guidance, the delivery system was introduced, and the angle between the device and the annulus plane was adjusted by catheter deflection and rotation, directing the tip of the clip device toward the target area.
Under ultrasound MPR mode, the anchoring component was deployed into the annulus. After confirming stable traction, the clamping arms were opened and apposed to the annulus. The anchoring component was then retracted to close the clamping arms and achieve annuloplasty.
A 14T K-Clip® and a 16T K-Clip® were implanted at the posteroseptal commissure and anteroposterior commissure respectively. After deployment of the two clips, additional clamping space was observed intraoperatively, so a third 14T K-Clip® was implanted at the posteroseptal region, closer to the septal side.
The procedural result was satisfactory, and the clip components were released.
First Clip: 14T clip at the posteroseptal commissure. Due to redundancy of the posterior leaflet hinge region with risk of perforation, the anchor was placed slightly toward the atrial side.
Delivery system entering RA via SCV
Opening clip arms, adjusting orientation, and apposing to the annulus
Retracting tissue, closing clip arms
Second Clip: Based on the effect after the first clip and the annular distance at the antero-posterior commissure, the 2nd implant was a 16T device clipping the antero-posterior commissure.
Clip oriented toward antero-posterior commissure
Identifying hinge region under MPR before anchoring screw
Adjust the orientation of the clamping arms, appose them to the annulus, and prepare for clamping.
Third Clip: There is remaining clamping space at the posterior leaflet near the septal side. Clamping at the posteroseptal commissure (annulus plane) can be attempted again. Perform clamping at the posteroseptal region following the same procedure.
Surgical Outcome
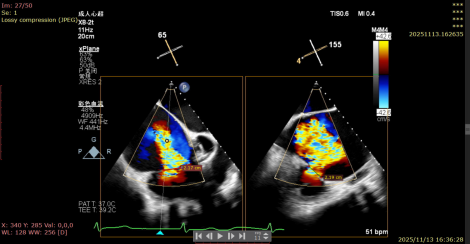
1.TR Reduction: Overall reduction greater than 3+ (decreased from massive 6+ to moderate-to-severe 3+).
Massive 6+
Moderate-to-Severe 3+
2.Annuloplasty Effect: Annular morphology remodeled, central gap significantly reduced.
Preoperative 3D
Postoperative 3D
Summary
The successful introduction and precise application of K-Clip® technology in Qingdao has not only opened up a new minimally invasive treatment pathway for high-risk patients with critical tricuspid regurgitation, but also signifies that the valvular intervention team of the Heart Center of Qingdao Municipal Hospital has reached an advanced national level in diagnosis and treatment.
In the future, the hospital will continue to be patient-centered, rely on the core advantages of multidisciplinary collaboration, and further deepen the field of interventional therapy for valvular heart disease. It will continuously explore the clinical application boundaries of domestic innovative devices, accumulate more experience in the diagnosis and treatment of complex cases, and bring cutting-edge technologies to benefit more cardiovascular patients in the region and even across the country. This will inject a steady stream of "Qingdao Strength" into promoting the standardized and precise development of valvular intervention in China.
Expert Profiles

Shao Yibing
Qingdao Municipal Hospital

Xia Wei
Qingdao Municipal Hospital

Niu Zhaozhuo
Qingdao Municipal Hospital

Chu Qiang
Qingdao Municipal Hospital

K-Clip® Transcatheter Tricuspid Annuloplasty System:
1. Transvascular puncture approach, minimally invasive, with an 18Fr outer sheath diameter.
2. Simple operation, all steps performed on the atrial side, short learning curve.
3. All steps reversible before deployment, ensuring controlled procedural outcomes.
4. Physiological annuloplasty technique, preserving native leaflets without damage.