K-Clip®+TEER: A Breakthrough in Minimally Invasive One-Stop Surgery
Recently, a team led by Professor Liu Jinping from the Cardiovascular Hospital of Zhongnan Hospital of Wuhan University, together with a team led by Professor Wang Bin from the Department of Ultrasound, has successfully performed a highly difficult minimally invasive cardiac surgery. For an elderly patient with complex valvular heart disease at high surgical risk, the procedure simultaneously implemented transcatheter tricuspid valve annuloplasty (TTVA) combined with transcatheter edge-to-edge mitral valve repair (TEER).The success of this surgery marks a new technological breakthrough achieved by the Cardiovascular Hospital of Zhongnan Hospital of Wuhan University in the field of minimally invasive interventional therapy for structural heart disease, especially in the management of complex multivalvular lesions.
Case Focus: Treatment Dilemmas of High-Risk Patients
The patient was an 82-year-old male admitted due to recurrent shortness of breath following physical activity and paroxysmal nocturnal dyspnea. He had a past medical history of hypertension, atrial fibrillation and heart failure.
Preoperative precise assessment by transthoracic and transesophageal echocardiography (TTE/TEE) revealed:
-
Mitral valve: severe functional regurgitation (4+), effective regurgitant orifice area (EROA) 0.52 cm², regurgitant volume 68 mL.
-
Tricuspid valve: Type IIIb quadricuspid malformation with insufficiency, secondary severe regurgitation (4+), mild annular dilatation (mean diameter 40 mm), mean vena contracta 10 mm. Regurgitant orifices are located at anteroseptal, central, and posteroseptal regions, with marked enlargement of the right atrium and right ventricle.
-
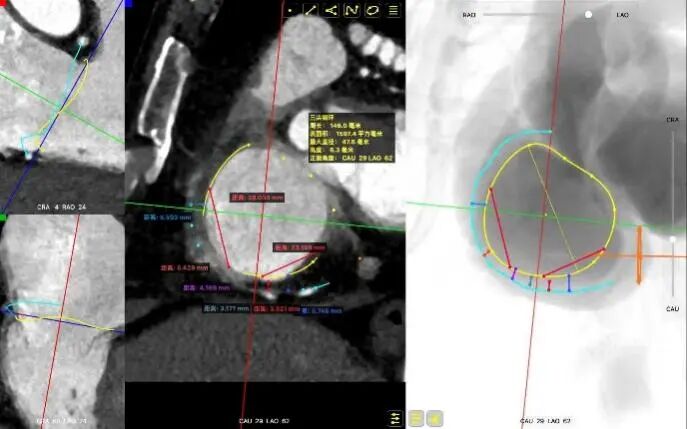
CTA: 31% systole: perimeter 135 mm, area 1373 mm²; 75% diastole: perimeter 146 mm, area 1597 mm².。
-
RCA-TA: The right coronary artery courses toward the atrial side at the anteroposterior commissure, relatively far from the annulus. At the posteroseptal commissure, the distance between the right coronary artery and the annulus is approximately 3 mm, with a low risk of compromising the right coronary artery.。
The patient's STS score indicated that he was at high risk for conventional surgery. Long-term heart failure resulted in poor quality of life, with NYHA functional class IV. He also had multiple comorbidities including persistent atrial fibrillation and pulmonary hypertension (estimated PASP 55 mmHg).
Core Decision: Multidisciplinary Heart Team Develops Individualized Minimally Invasive Strategy
Faced with the challenges of advanced age and intolerance to conventional open-heart surgery with cardiopulmonary bypass, the heart team at the Cardiovascular Hospital of Zhongnan Hospital of Wuhan University conducted a multidisciplinary discussion. The team unanimously agreed that the key to the patient's treatment lies in:
1.Mitral and tricuspid regurgitation must be managed concomitantly to break the vicious cycle of heart failure.
2.The least invasive surgical approach must be adopted to reduce perioperative risks.
After a comprehensive assessment, the team led by Professor Liu Jinping, including Professor Zhang Li and Doctor Chen Xing, ultimately determined a one-stop transcatheter minimally invasive solution: via a vascular puncture approach, the edge-to-edge clip repair of the mitral valve and the annuloplasty constriction of the tricuspid valve were successively performed in a single operation.
Surgical Procedure: Technical Implementation with Precise Multidisciplinary Collaboration
The operation was performed in a hybrid operating room and completed under the guidance of real-time three-dimensional transesophageal echocardiography (3D TEE) and X-ray fluoroscopy throughout the entire process.
Surgeon team: Professor Liu Jinping's team including Professor Zhang Li and Doctor Chen Xing
Ultrasound guidance: Professor Wang Bin's team including Professor He Jun
Mitral Valve Repair Stage: Via the transfemoral venous approach, a 4.0 cm atrial septal puncture was performed, and one mitral valve clip was selected. The unique feature of wide-angle deployment effectively resolved the issue of excessive leaflet tension during valve clip closure. Under the precise guidance of ultrasound, one clip was successfully implanted at the site of the widest regurgitation in the A2-P2 segment of the mitral valve. Immediate postoperative TEE assessment showed that mitral regurgitation was reduced to trivial (1+), the mean transvalvular pressure gradient was only 3 mmHg, and pulmonary venous retrograde flow was significantly improved.
Preoperative Imaging
Mitral regurgitation
3D color Doppler
Mitral valve Zone 2
Color Doppler of Mitral valve Zone 2
Intraoperative Imaging
Atrial Septal Puncture
Guide Sheath Implantation
Mitral Clip Trajectory Test
Orientation Confirmation
Orientation Reconfirmation After Transvalvular Crossing
Clip Closure Following Leaflet Capture
Regurgitation Essentially Eliminated at 25° Closure
Trivial Residual Regurgitation Post Deployment
Stable Tissue Bridge
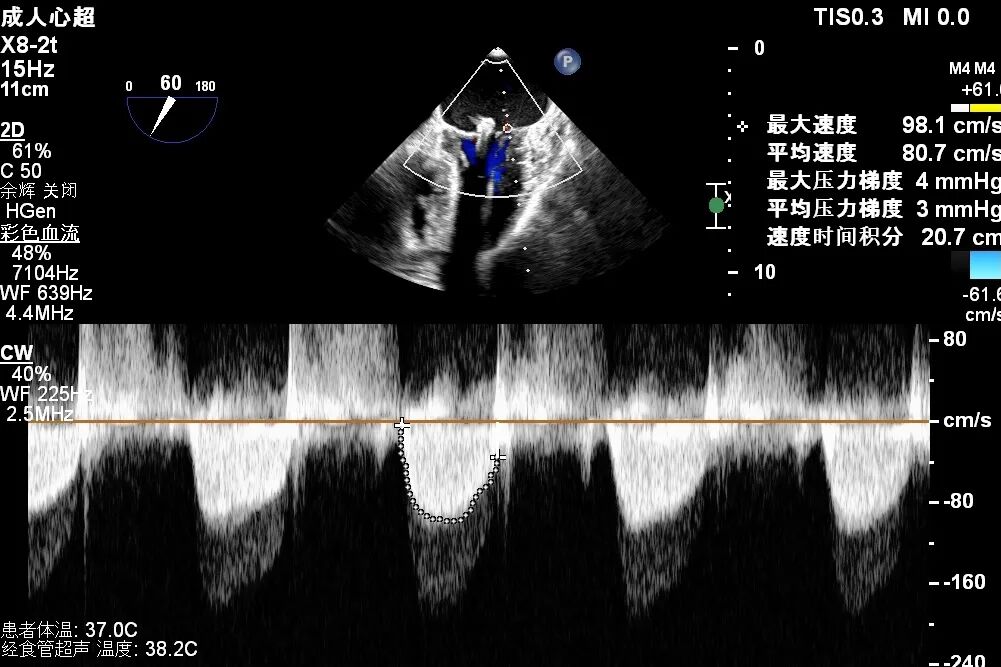
Transvalvular Pressure Gradient of 3 mmHg
Tricuspid Valve Annuloplasty Stage:Subsequently, via the right internal jugular vein approach, the K-clip® transcatheter tricuspid valve annuloplasty system was delivered to the right atrium. With the assistance of three-dimensional ultrasound stereoscopic views, a 12T clip was successfully implanted at the posteroseptal commissural annulus of the tricuspid valve, and a 14T clip at the anteroposterior commissural annulus, achieving effective constriction of the dilated annulus. Immediate postoperative assessment demonstrated that tricuspid regurgitation was improved from severe (4+) to mild (1+) instantaneously.
The operation proceeded smoothly with a total duration of approximately 3.5 hours. The patient's vital signs remained stable intraoperatively, and no blood transfusion was required.
1.Intraoperative baseline assessment of regurgitation severity
2.Placement of large sheath and delivery system under ultrasound guidance
3.Steer and rotate the delivery system to target the lesion, and implant the anchor screw via the 3D MPR plane
4.Land the clamping arms after orientation adjustment, and close the clamping arms slowly
5.Perform the same procedure for the second clip; the clip morphology is stable under 3D imaging
Surgical Outcome


Annuloplasty Effect: The tricuspid valve annulus area was reduced from 9.96 cm² to 4.6 cm², representing a 53% decrease in annulus area.
Preoperative regurgitation (severe)
Postoperative regurgitation (trivial)
Surgical Outcome: Severe tricuspid regurgitation (4+) was reduced to mild tricuspid regurgitation (1+).
Postoperative Outcome: Hemodynamics and cardiac function improved significantly.
-
Immediate Outcome:The patient experienced immediate relief of dyspnea and stable hemodynamics right after the surgery.
-
Short-term Recovery:The endotracheal tube was removed within 24 hours postoperatively, the ICU stay lasted 2 days, and the patient was discharged from hospital upon recovery on the 7th postoperative day.
-
Follow-up Data:A follow-up TTE performed 1-month postoperative follow-up showed that mitral and tricuspid regurgitation remained stably at mild levels; the left and right ventricular internal diameters were significantly reduced compared with preoperative measurements; the NYHA cardiac function class improved from Class Ⅳ to Class Ⅱ. The patient’s exercise tolerance was markedly enhanced, and the quality of life was fundamentally improved.
Academic Value and Significance of Regional Leadership
The successful performance of this surgery fully demonstrates the comprehensive strength of the Department of Cardiovascular Surgery at the Cardiovascular Hospital of Zhongnan Hospital of Wuhan University in the field of complex structural heart disease treatment:
1.Technology integration capability: We have successfully integrated and applied two of the world’s cutting-edge transcatheter valve repair and annuloplasty technologies to the same high-risk patient, achieving a genuine "minimally invasive double valve repair".
2.Multidisciplinary collaboration model: The efficient collaboration of the Heart Team is the cornerstone of the surgical success. From precise preoperative assessment and treatment protocol formulation to intraoperative ultrasound guidance and anesthetic management, it embodies a patient-centered modern medical model.
3.Expanding the boundaries of treatment: It provides a new, safe and effective treatment option for patients with complex double valve disease who were excluded from traditional open surgery due to advanced age, multiple comorbidities and poor cardiac function.
The completion of this highly complex surgery has consolidated the leading position of the Cardiovascular Hospital of Zhongnan Hospital of Wuhan University in minimally invasive interventional treatment for valvular heart disease in Central China, and also demonstrated our determination and capability to localize internationally advanced medical technologies and serve a large number of critically ill patients.
Department Profile
The Department of Cardiovascular Surgery at Zhongnan Hospital of Wuhan University is a National Key Clinical Specialty, boasting distinctive strengths in the minimally invasive surgery, hybrid surgery and treatment of end-stage heart diseases for cardiothoracic vascular disorders. The department routinely performs a full range of advanced procedures including minimally invasive valvuloplasty/valve replacement, transcatheter aortic valve replacement (TAVR), transcatheter edge-to-edge repair (TEER), and minimally invasive coronary artery bypass grafting (CABG), striving to deliver optimal therapeutic outcomes for patients with minimal trauma.
Expert Profile




K-Clip® Transcatheter Tricuspid Annuloplasty System:
1、Vascular puncture approach with minimal trauma and an 18Fr outer diameter sheath.
2、Simple operation, all procedures completed at the atrial surface, with a short learning curve.
3、All procedural steps are reversible before detachment, enabling controllable surgical outcomes.
4、Physiological annuloplasty technology that preserves the native valve leaflets without damage.