First case in Southwest China! TTVA + TEER | The First People's Hospital of Yunnan Province successfully performed a one-stop procedure using two domestic devices
Recently, the valvular heart disease team of the Department of Cardiology led by Chief Physician Pang Mingjie from The First People's Hospital of Yunnan Province successfully completed a one-stop interventional procedure for a high-risk complex patient with severe mitral regurgitation (MR) combined with extremely severe tricuspid regurgitation (TR). The operation was carried out with close collaboration among the Department of Anesthesiology, Echocardiography Laboratory, Cardiac Catheterization Laboratory, Cardiac Care Unit (CCU) and nursing teams. The patient suffered from secondary severe mitral regurgitation and extremely severe tricuspid insufficiency, accompanied by recurrent heart failure with poor response to medical therapy. The patient also had a medical history of hypertension, atrial fibrillation, cerebral infarction and recurrent vaginal bleeding, presenting with a critical and complicated clinical condition.

After multidisciplinary team (MDT) discussion, the patient was deemed to have surgical indications but was not a candidate for open surgery. Following thorough assessment of the mitral and tricuspid valve anatomy revealed by echocardiography and with informed consent obtained from the patient and her family, the medical team decided to perform transcatheter edge-to-edge repair of the mitral valve (DragonFly™-TEER) combined with concurrent transcatheter tricuspid valve annuloplasty (K-Clip®). The procedure was successfully completed with close cooperation of the valvular heart disease team. Postoperatively, both mitral and tricuspid regurgitation were reduced to mild grade, and the patient’s heart failure symptoms improved remarkably, creating favorable conditions for her subsequent gynecological surgery. The successful completion of this one-stop dual-valve interventional repair marks a new breakthrough in the field of transcatheter interventional therapy for valvular heart disease in our hospital. It also provides a feasible, safe and effective new treatment option for more elderly, high-risk patients with complex valvular heart disease complicated by multiple comorbidities.

Patient Basic Information
Gender: Female, Age: 67 years old
The patient was admitted due to recurrent dyspnea and intermittent bilateral lower limb edema. Past medical history: The patient has had hypertension for many years with irregular medication use. She was diagnosed with cerebral infarction two years ago presenting with facial deviation. Recurrent unexplained vaginal bleeding has occurred over the past month, and gynecological surgery is scheduled. Electrocardiogram revealed persistent atrial fibrillation. Post-admission echocardiography showed marked bilateral atrial enlargement, moderate to severe mitral regurgitation and severe tricuspid regurgitation.
Preoperative Evaluation of the Mitral Valve
Severe mitral insufficiency (MR 4+), functional mitral regurgitation (FMR). Regurgitation is mainly originated from segment 2 with central regurgitant jet. During systole, the anterior and posterior mitral leaflets are nearly at the annular plane, with a low leaflet-to-annulus index. Interatrial septum presents with paradoxical motion and significant mitral annular dilatation is noted.
Preoperative Evaluation of the Tricuspid Valve
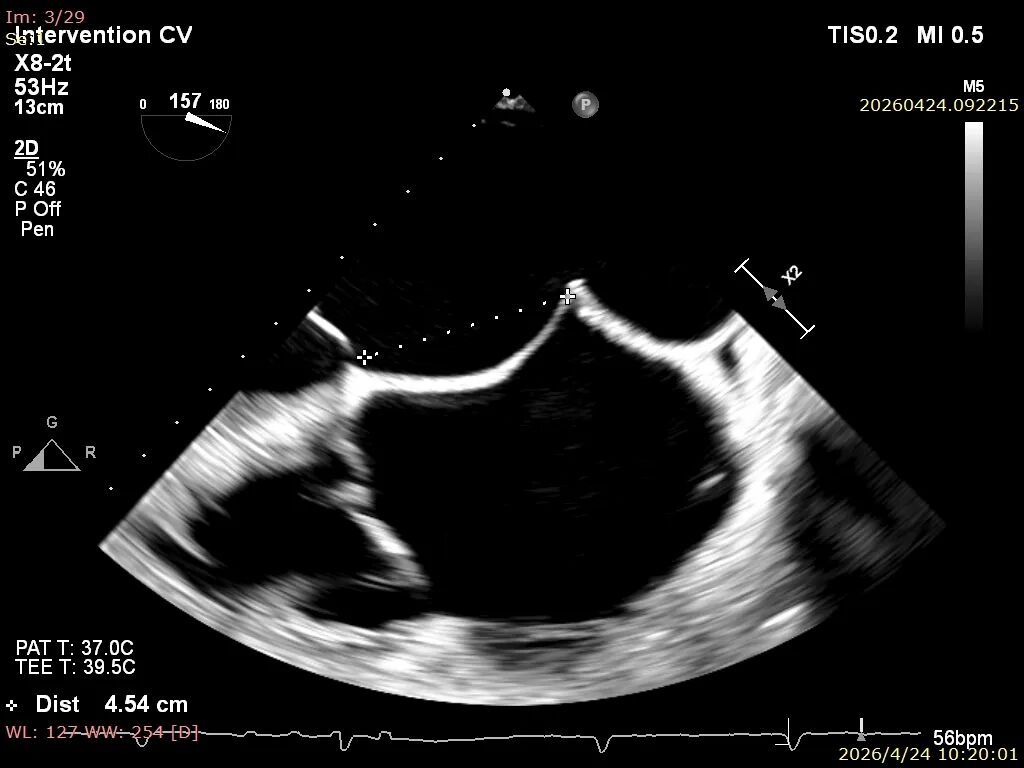
Intraoperative transesophageal echocardiography (TEE) assessment before procedure: Severe tricuspid regurgitation (4+), with a mean vena contracta width of 9 mm. Regurgitant orifices are located at the anteroseptal, central and posteroseptal regions. A 4 mm gap is detected at the central portion. Marked tricuspid annular dilatation is present with a mean annular diameter of 47 mm. The patient has persistent atrial fibrillation.
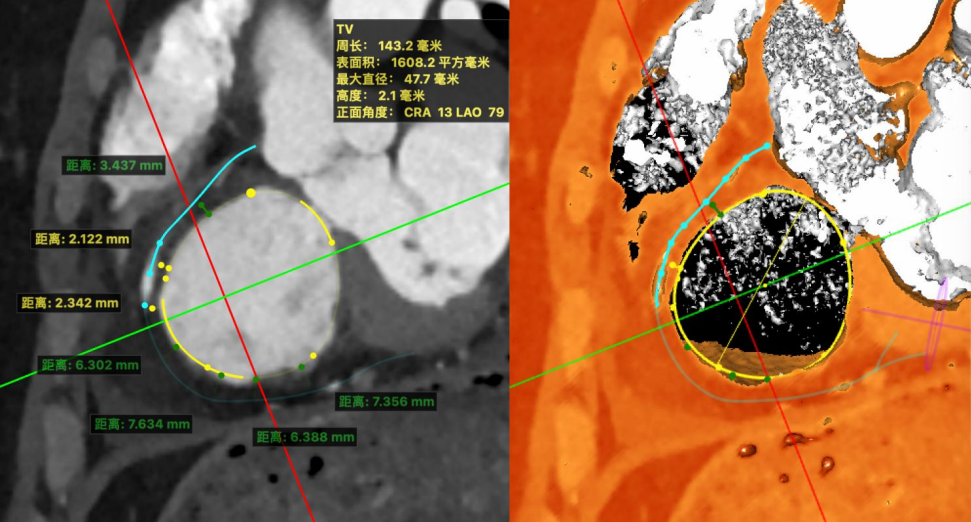
Preoperative CT assessment: Systolic circumference: 143 mm, area: 1608 mm². Non-right dominant coronary circulation. The coronary course at the anteroposterior junction aligns with the valvular annulus, while the remaining segments course toward the atrium, which may pose potential procedural impacts.
Surgical Strategy
1.First, perform transcatheter mitral edge-to-edge repair (DragonFly™-TEER). The interatrial septum of the patient may have poor support, leading to height loss after transseptal puncture. Therefore, a sufficient puncture height (>4.5 cm) is required. Given the significant mitral annular dilatation, attention should be paid to leaflet tension during clip closure to reduce the risk of leaflet injury. One XW0612 clip was deployed at segment 2. Additional clip placement was determined intraoperatively based on residual regurgitation and transvalvular pressure gradient. Specifically, one 0612 clip was implanted at segment 2, and one 0609 clip was deployed laterally if necessary. After clip deployment, regurgitation was reduced to mild to moderate, with the mean transvalvular pressure gradient below 5 mmHg. Upon completion of TEER and confirmation of stable hemodynamics, transcatheter tricuspid valve annuloplasty with K-Clip® was subsequently performed via the internal jugular vein approach.
2. After conducting multi-dimensional assessments of the tricuspid annulus and the distance between the right coronary artery and the annulus, we formulated a precise treatment plan centered on implantation of three K-Clip® devices, taking full account of the patient's lesion characteristics, anatomical details and coronary artery-related influencing factors. During the procedure, a 14T K-Clip® was implanted at the posteroseptal junction of the tricuspid valve, a 12T K-Clip® was deployed on the posterior leaflet, and another 14T K-Clip® was placed at the anteroposterior junction of the tricuspid valve. This three-point positioning implantation technique can effectively reduce the tricuspid annular diameter and improve leaflet coaptation, directly correcting tricuspid regurgitation anatomically and providing crucial structural support for the patient's smooth postoperative recovery.
Procedure of M-TEER
Preoperative
Commissural view
Poor coaptation of the anterior and posterior leaflets at segment 2.
3D
3D color
Procedure
Transseptal puncture height: 4.5 cm
Guide sheath placement
Deploy the DragonFly™ XW0612 valve clip
Adjust the trajectory and axis
Advance below the valve and grasp the leaflets
Gripper lowered, obvious bouncing of anterior and posterior leaflets
Close the valve clip, with residual functional regurgitation at the lateral side
Deploy one DragonFly™ SW0609 valve clip at the lateral side
Leaflets captured with significant leaflet bouncing
After releasing the valve clip, regurgitation was reduced to mild to moderate
Stable tissue bridge confirmed on 3D assessment
Final regurgitation decreased from severe to mild to moderate
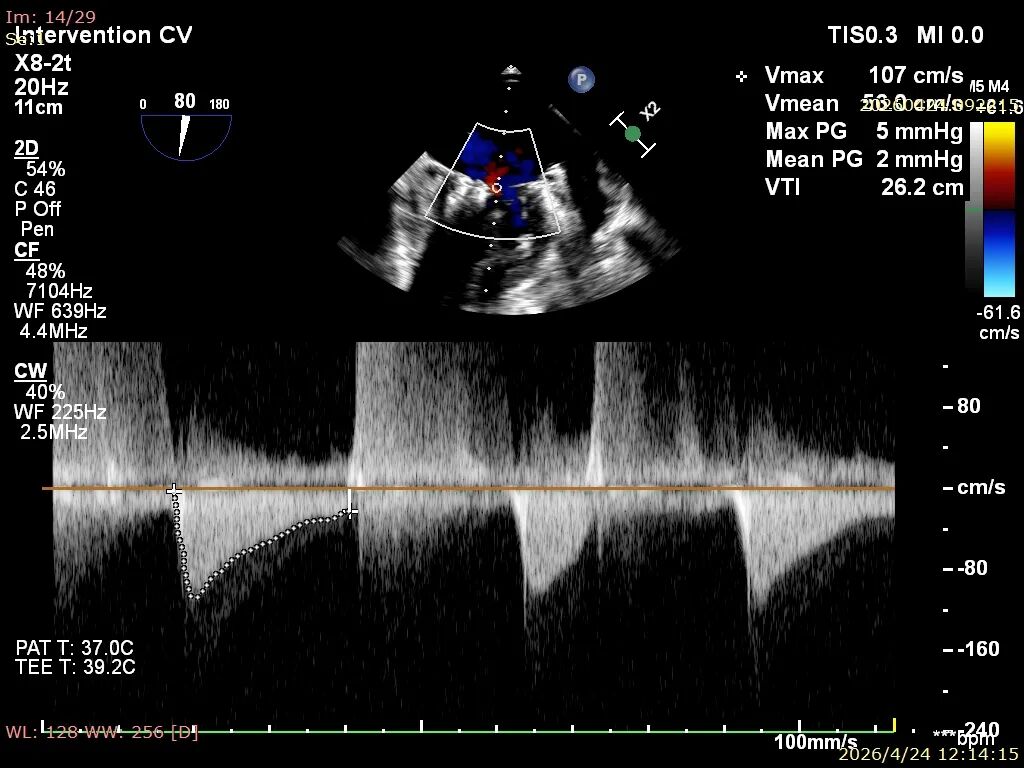
TMPG:2mmHg
Procedure of K-Clip®
Baseline regurgitation after anesthesia
Baseline after anesthesia
1.The first 14T clip was directed toward the posteroseptal commissure of the tricuspid valve
The MPR device was aligned to the posteroseptal region
2. Screw anchoring: The screw was driven into the tricuspid annulus
3. Prepare for clipping: Adjust the orientation
The MultiVue was apposed to the annulus and the clipping component was closed
MultiVue apposed to the annulus
The third clip was positioned against the annulus via MultiVue, and the clipping component was closed
5. The second set of devices was operated in the same manner. The 12T clip was positioned near the anteroposterior commissure
The second clip was positioned near the anteroposterior commissure
6. Anchoring screw deployment: The screw was driven into the tricuspid annulus
Second MultiVue anchored the annulus
7. Prepare for clipping: Adjust orientation
Second clip: MPR adjusted orientation to align with the annulus
8. MultiVue apposed to the annulus and clipping component closed
9. The third 14T clip was deployed across the anteroposterior commissure
10.The third 14T clip was directed toward the anteroposterior commissure of the tricuspid valve
Third clip aligned with the anteroposterior commissure
Evaluation of surgical outcomes
Regurgitation assessment: Reduced from grade 5+ preoperatively to grade 2+.
Preoperative:
Central regurgitation preoperatively
Postoperative:
Postoperative central regurgitation
No abnormal morphology after deployment of three clips under DSA. All anchoring sites were at the intended positions, and RCA blood flow was unaffected

Summary
The successful completion of this procedure marks Yunnan’s entry into the era of one-stage minimally invasive dual-valve intervention. The Department of Cardiology of The First People’s Hospital of Yunnan Province now possesses the comprehensive capability for one-stop interventional treatment of severe lesions involving both left and right cardiac valves. The hospital’s cardiac valve team has long independently performed a range of sophisticated interventional procedures, including transcatheter aortic valve replacement (TAVR), transcatheter edge-to-edge repair (TEER) for mitral valve, and tricuspid valvuloplasty with K-Clip system. The success of this one-stage dual-valve procedure serves as a major milestone, advancing the technical portfolio from single-valve repair to combined valvular intervention. Moving forward, the team will continue to refine minimally invasive interventional techniques for valvular heart disease and explore more precise and safer treatment regimens, enabling more patients to benefit from cutting-edge medical advances
Expert Profile

Pang Mingjie
The First People’s Hospital of Yunnan Province
Chief Physician, Doctoral Supervisor. He is a Young and Middle-aged Academic and Technical Leader of Yunnan Province, an Outstanding Professional and Technical Talent with Outstanding Contributions in Yunnan Province, a Distinguished Physician of the National Ten-Thousand Talents Program, and a Medical Discipline Leader of Yunnan Province. He serves as an evaluation expert for the Academic Degrees Center of the Ministry of Education, a reviewer for the National Natural Science Foundation of China, Vice Chairman of the Yunnan Professional Committee for Cardiac Critical Care, and Vice Chairman of the Cardiology Committee of Yunnan Hospital Association. He also acts as a scientific and technological evaluation expert for science and technology departments of Guangdong and other six provinces and municipalities. His main research focus is interventional diagnosis and treatment of coronary heart disease and valvular heart disease. He has won the Second and Third Prizes of Science and Technology Achievement Awards issued by Yunnan Provincial People's Government and Yunnan Health Commission for ten research achievements. Eight research projects have been funded by the National Natural Science Foundation of China and Yunnan Provincial Natural Science Foundation. As the first author, he has published more than 40 papers in Chinese core journals and over 10 SCI papers. Additionally, he works as a peer reviewer for multiple academic journals.

Lu Can
The First People’s Hospital of Yunnan Province
Associate Chief Physician, Department of Cardiology, The First People’s Hospital of Yunnan Province. Member of the Cardiac Health Committee of China Intelligent Engineering Research Association, Member of the Cardiovascular Disease Prevention and Rehabilitation Branch of Yunnan Preventive Medicine Association, and Tutor of the Training Base for Restricted Medical Technologies in Yunnan Province. He was a visiting scholar at Princeton Cardiovascular Center in the United States and University Hospital Magdeburg in Germany. He has long been engaged in the diagnosis and treatment of hypertension, heart failure, hyperlipidemia and other diseases, and specializes in interventional therapy for coronary heart disease and valvular heart disease. He has participated in one project funded by the National Natural Science Foundation of China and two provincial joint special projects, and published multiple SCI papers and monographs. He won the championship in the final of the 2019 Great Wall International Congress of Cardiology National Competition for Young and Middle-aged Cardiovascular Physicians, and the Gold Award of the 2024 Yunnan Red Cross Public Welfare Competition. In 2024, he served as the team leader of the medical assistance team dispatched to Luang Prabang, Laos.

Ding Xiaoxue
The First People’s Hospital of Yunnan Province
She graduated from the eight-year integrated Bachelor-Master-PhD program in Clinical Medicine at Xiangya School of Medicine, Central South University in 2012. Since graduation, she has been engaged in clinical work in the Department of Cardiology, The First People’s Hospital of Yunnan Province, and obtained the qualification of Attending Physician in 2015.Up to now, she has published one core journal article as the first author, and participated in the publication of two core journal articles and one SCI article. She has presided over one joint special project of Yunnan Provincial Science and Technology Department and Kunming Medical University, and participated in one project supported by the National Natural Science Foundation of China.

Li Lijiang
The First People’s Hospital of Yunnan Province
Attending Physician, Master of Medicine, Department of Cardiology, The First People’s Hospital of Yunnan Province
She has been working in the Department of Cardiology of the hospital since 2012, engaging in frontline clinical practice for years and once served as the teaching secretary of the department. Her main work covers interventional procedures for coronary heart disease and valvular heart disease, as well as postoperative follow-up of valvular disease patients.

Zhai Jiaming
The First People’s Hospital of Yunnan Province
Attending Physician, Master of Medicine.He specializes in the diagnosis and treatment of cardiovascular diseases. He has long been engaged in minimally invasive interventional therapy for coronary heart disease and structural heart diseases (including congenital heart disease and valvular heart disease). He is proficient in echocardiography and peripheral vascular ultrasonography.

Su Wenhua
The First People’s Hospital of Yunnan Province
Attending Physician, Department of Cardiology. He graduated from Kunming Medical University in 2015 and has since worked at the Department of Cardiology, The First People’s Hospital of Yunnan Province. His main focus is on the interventional diagnosis and treatment of coronary heart disease and structural heart disease.

K-Clip® Transcatheter Tricuspid Annuloplasty System:
1.Vascular puncture approach with minimal trauma and an 18Fr outer diameter sheath.
2.Simple operation, all procedures completed at the atrial surface, with a short learning curve.
3.All procedural steps are reversible before detachment, enabling controllable surgical outcomes.
4.Physiological annuloplasty technology that preserves the native valve leaflets without damage.